
Article Series
Autoclaving leaves 10% of your clinical waste untreated and sends the rest to landfill. For operators already familiar with non-incineration medical waste treatment, this article dives into the head-to-head technical comparison between autoclaving and subcritical water hydrolysis — covering operating parameters, waste stream compatibility, residue output, and total cost trajectory through 2028.

How Does Autoclave Temperature Compare to Subcritical Water Hydrolysis?
Subcritical water hydrolysis operates at 200°C and 20 bar pressure — 66°C hotter than the maximum autoclave cycle. That temperature gap is the difference between sterilising waste and breaking it down at a molecular level.

- Autoclaves run at 121–134°C and 1–3 bar, killing most bacteria through pressurised steam contact over 30–90 minutes
- SWH runs at 200°C and 20 bar, triggering hydrolytic decomposition of organic compounds — not just surface sterilisation
- Autoclave output is shredded, sterilised waste that still requires landfill disposal at £126.15/t (~$160/t) in 2025/26
- SWH output is a sterile, volume-reduced residue with potential soil amendment value — diverting material from landfill entirely
- Both technologies complete a cycle in approximately 30 minutes, but SWH processes a broader range of waste streams per cycle
This applies when you are processing infectious clinical waste (orange bag, HTM 07-01) and comparing real operating parameters. It does not apply if you are evaluating waste streams that require incineration by law, such as anatomical waste.
Micro-example: A 400-bed NHS acute trust generating 12 tonnes of orange-bag waste per month runs an autoclave at 134°C. Every tonne of autoclaved residue still goes to landfill at £126.15/t — costing £1,513.80/month in landfill tax alone. The same 12 tonnes processed through SWH at 200°C produces a sterile residue classified for land application, eliminating that landfill cost entirely.
Can Subcritical Water Hydrolysis Meet HTM 07-01 Compliance Without Incineration?
Yes — and it does so with a higher validation standard than most autoclaves achieve. PHANTOM's subcritical water hydrolysis holds ISTAATT Level III certification, which establishes treatment equivalence to incineration for non-incineration pathways under HTM 07-01. UK operators register a PHANTOM unit under an Environmental Permit issued by the EA, SEPA, or NRW — with no secondary incineration contract required.
- ISTAATT Level III = Log-6 reduction across all relevant HTM 07-01 clinical waste microbiological groups — the same destruction benchmark as incineration
- Environmental Permit required: Environment Agency (England), SEPA (Scotland), NRW (Wales) — PHANTOM installations typically register under a bespoke waste treatment permit
- No trade effluent consent is required for PHANTOM's liquid output in most standard EA permit templates
- Permit application timeline: 4–6 months for a standard installation with pre-application EA consultation
- NHS England's 2023 Clinical Waste Strategy explicitly supports alternative treatment technologies as part of its 15% cost-reduction target by 2030
For the full permit application timeline and EA pre-application process, see our guide to UK on-site medical waste treatment permits and validation.
This applies to operators in England, Scotland, and Wales seeking EA/SEPA/NRW approval to treat yellow-bag, orange-bag, and anatomical waste on-site under HTM 07-01 streams. It does not apply to cytotoxic and cytostatic (purple bag) waste — that stream requires specialist incineration and cannot be processed through subcritical water hydrolysis under current EA guidance.
Micro-example: An independent dialysis centre in Leeds applied for an EA on-site treatment permit for a PHANTOM unit in Q1 2024. The permit was granted in under five months based on the ISTAATT Level III validation certificate and a pre-application meeting with the EA area team. The unit now handles all sharps-free clinical waste from three satellite clinic sites — replacing a £420/t (~$533/t) external contract with no incineration dependency.
Which Waste Streams Can an Autoclave NOT Process?
Autoclaves cannot treat approximately 10% of clinical waste. That 10% includes the most dangerous and expensive categories in the hospital waste stream.
- Prion-contaminated waste (CJD): Standard autoclaving at 134°C fails to completely denature prion proteins. CJD-contaminated material resists steam sterilisation and remains highly infectious post-treatment
- Cytotoxic and chemotherapy waste: Active chemical compounds survive steam sterilisation temperatures. HTM 07-01 requires incineration for all cytotoxic waste
- Pharmaceutical waste: Drug compounds are not deactivated by steam alone. Autoclaving pharmaceutical waste creates a disposal liability, not a solution
- Anatomical and pathological waste: Not approved for autoclave treatment under UK regulations
- Chemical aerosolisation risk: Autoclaves can aerosolise chemical compounds present in mixed waste, creating secondary contamination
This applies when you are evaluating whether a single on-site treatment system can handle your full clinical waste profile. It does not apply if your facility generates only standard infectious waste with no pharmaceutical or cytotoxic streams.
Micro-example: A regional cancer treatment centre generates 2.4 tonnes of cytotoxic waste per month alongside 8 tonnes of standard infectious waste. The autoclave handles the 8 tonnes — but the 2.4 tonnes of cytotoxic waste still ships to incineration at £617/t (~$783/t). That is £1,480.80/month in incineration fees for waste the autoclave physically cannot touch.
What Does the True Cost of Autoclaving Include?
On-site SWH consistently undercuts the combined cost of an autoclave-plus-incineration hybrid model once cytotoxic and anatomical fractions are included. The true cost of autoclaving is never just the autoclave — it is the autoclave for compliant streams, plus incineration for excluded streams, plus haulage, plus contractor management across two separate frameworks.
- Capital: NHS Supply Chain framework autoclave units range from approximately £35,000 (~$44,450) for 150L laboratory-grade models to £45,000+ (~$57,150+) for large-capacity units. Full acute trust throughput typically requires multiple units operating in parallel.
- Operating: Medical-grade autoclaves consume thousands of litres of water and significant electrical energy per day — independent of actual throughput volumes.
- Excluded stream cost: Any waste streams prohibited from autoclave treatment still require incineration at approximately £617/tonne (~$783/tonne) — making a hybrid contractor model the operational default for most acute trusts.
- UK ETS uplift from 2028: Incineration gate fees are projected to increase by approximately £48/tonne as waste-to-energy facilities enter the UK Emissions Trading Scheme. A trust sending 1,000 tonnes/year to incineration faces an additional £48,000/year (~$60,960/year) in treatment cost from 2028 with no change in volume.
- PHANTOM SWH on-site TCO: Eliminates haulage costs, reduces contractor exposure, and processes the full compatible stream in a single treatment cycle. See the PHANTOM organic waste treatment machine for throughput specifications across the 0.5t, 1t, 2t, and 3t models.
This applies when modelling procurement decisions for NHS trusts with mixed clinical waste streams above 10 tonnes/week. It does not apply to GP practices or small community settings generating under 2 tonnes/month — at that volume, off-site contractor economics remain more favourable.
Micro-example: A medium acute trust generating 800 tonnes/year of clinical waste — with 200 tonnes going to incineration at £617/t (~$783/t), costing £123,400/year (~$156,718/year) — faces a projected ETS-adjusted incineration cost of approximately £170,000/year (~$215,900/year) by 2029 for that fraction alone. The autoclave handles the compliant fraction, but the incineration tail keeps growing.
What Happens to the Residue After Each Treatment?
Autoclave residue goes to landfill. SWH residue has potential value as a soil amendment. That distinction changes the entire cost equation.
- Autoclaved waste is shredded and sterilised but not decomposed — it retains its original mass minus moisture, sent to landfill at £126.15/t rising to £130.75/t (~$166/t) from April 2026
- SWH residue is hydrolysed into a sterile, homogeneous material with reduced volume and mass — classified for potential land application rather than landfill
- Autoclaved sharps containers, plastics, and packaging retain their physical form — they occupy landfill space unchanged
- SWH breaks down organic polymers into simpler compounds, reducing total waste volume by up to 80%
- The liquid fraction from SWH contains recoverable nutrients, creating a potential revenue stream rather than a disposal cost
This applies when you are comparing total disposal cost over a 5-year contract. It does not apply if your primary concern is single-cycle throughput speed alone.
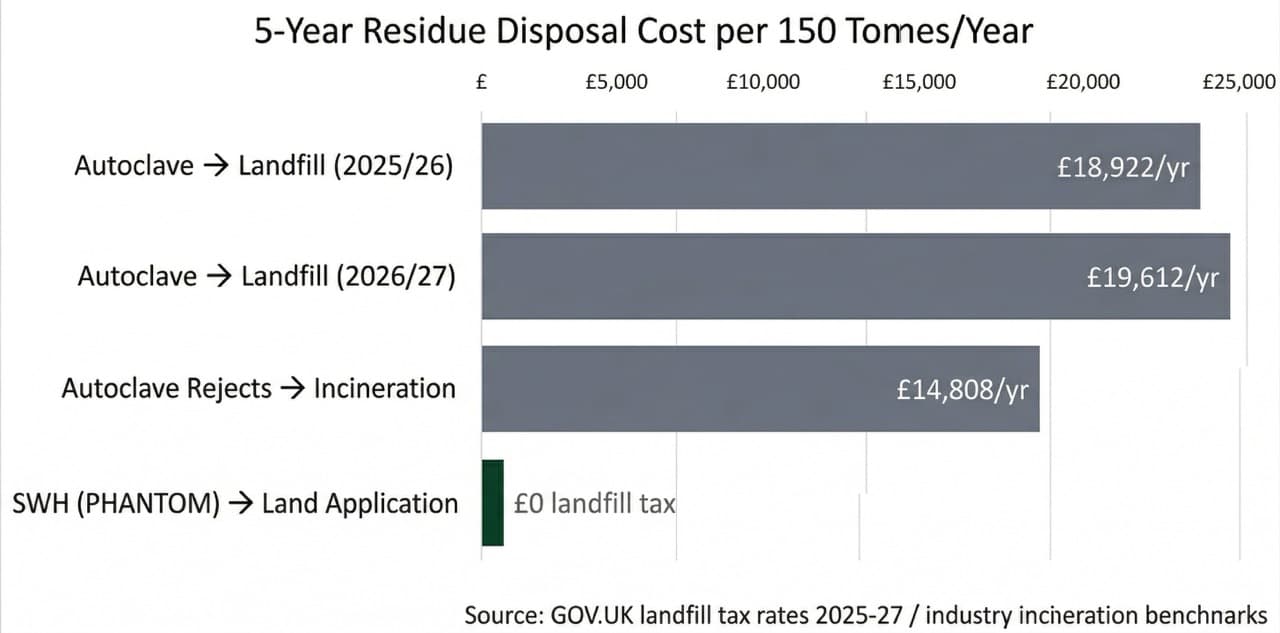
Micro-example: An NHS trust disposing of 150 tonnes of autoclaved residue per year pays £18,922/year (~$24,030/year) in landfill tax alone at £126.15/t. Over a 5-year contract, that is £94,612 in tax on waste that was already "treated." With landfill tax rising to £130.75/t from April 2026, the annual cost increases to £19,612/year — and the trajectory only steepens.
For a detailed financial model comparing all three treatment pathways, see the medical waste TCO comparison: autoclave vs incineration vs hydrolysis guide.
Does Autoclave Performance Degrade With Wet Clinical Waste?
Yes — and most facilities don't discover this until an audit. Autoclaves rely on dry saturated steam making uniform contact with the waste load. When clinical waste arrives with high moisture content — which is standard for NHS mixed-stream collections — steam penetration becomes uneven. The result is localised cold spots in the chamber where the thermal kill log falls short of the required Log-6, voiding the validation.
- Standard porous load autoclaves are validated for loads with moisture content below specified thresholds; NHS clinical waste routinely arrives at 60–75% moisture by weight
- Wet loads absorb steam and reduce chamber temperature before the holding time begins — shortening the effective kill period
- BS EN 285 validation tests are run with defined challenge loads; real-world wet mixed waste regularly deviates from those parameters
- Facilities running regular wet loads often pass quarterly validation tests (which use controlled loads) while under-performing on live cycles
- Discovery typically happens during an unannounced EA inspection or a post-incident root cause audit — not during routine operation
This applies when you are running an autoclave on mixed clinical waste streams from ward collections, community care, or multi-site consolidation. It does not apply to benchtop autoclaves used solely for instrument sterilisation, where load moisture is controlled.
Micro-example: In my experience commissioning a PHANTOM unit at a rural NHS community hospital with no contract haulage available, the most significant discovery was moisture tolerance. The site's clinical waste averaged 72% water content by weight. The previous autoclave had been consistently under-performing its validation log-kills because of wet load distribution — a finding that only emerged during a post-market audit two years into operation. PHANTOM's pressurised liquid environment made waste moisture content operationally irrelevant: there is no steam penetration problem when the entire process medium is pressurised water at 200°C.
How Will UK ETS Carbon Pricing Change the Cost of Incineration by 2028?
From 2028, every UK waste incineration facility will surrender carbon allowances under the UK Emissions Trading Scheme. Industry estimates project gate fee increases of approximately £48/t.
- January 2026: Voluntary Monitoring, Reporting and Verification (MRV) begins for all energy-from-waste and waste incineration operators
- 2028: Full UK ETS compliance — operators must purchase and surrender carbon allowances for fossil-derived emissions (primarily plastics in waste stream)
- Estimated gate fee increase: ~£48/t, pushing yellow-bag clinical waste incineration from ~£617/t (~$783/t) toward £665/t (~$844/t)
- Facilities relying on incineration for their autoclave reject stream (cytotoxic, pharmaceutical, prion waste) will absorb this increase directly
- SWH produces zero combustion emissions — it sits entirely outside the UK ETS scope
This applies when you are planning waste infrastructure investment with a 5–10 year horizon. It does not apply if you are evaluating treatment options for a single waste audit cycle.
Leading clinical waste contractors including Stericycle and Tradebe charge £480–£617/tonne (~$609–$783/t) for collection and incineration of Category B infectious waste under standard NHS framework agreements (source: NHS Supply Chain framework agreements, 2025/26 rates). UK ETS compliance from 2028 pushes that ceiling toward £665/t (~$844/t).
Micro-example: A private hospital group operating 6 facilities sends a combined 180 tonnes of clinical waste to incineration annually. At current rates (~£617/t), that costs £111,060/year (~$141,046/year). Post-2028 UK ETS compliance adds ~£48/t, pushing annual costs to £119,700/year — an £8,640 (~$10,973) increase with no change in waste volume or service level.

What Does HTM 07-01 Require From NHS Trusts Choosing Treatment Technology?
Under the 2024 DHSC update to HTM 07-01, NHS providers must demonstrate active accountability for waste stream segregation and treatment choice. The NHS segregation target of 20% HTI / 20% AT / 60% offensive waste creates a structural incentive to maximise alternative treatment throughput — but the guidance also mandates strict stream separation before any AT method is applied.
- Autoclave is classified as an Alternative Treatment (AT) method, approved for orange-stream infectious waste only under standard configurations
- NHS providers must report segregation performance against the 20:20:60 HTI:AT:OW ratio targets in their waste returns
- On-site alternative treatment — including SWH — requires an EA Environmental Permit (or equivalent SEPA/NRW authorisation in Scotland/Wales) applied for and granted before treatment begins
- HTM 07-01 defines performance requirements, not specific approved technologies. SWH is not prohibited — it must demonstrate the same sterilisation performance standards as any other AT method, evidenced by an appropriate validation certificate
- The 2024 update explicitly requires facilities to document the rationale for treatment technology choices, including environmental impact assessment
This applies to all NHS-registered healthcare providers in England. It does not apply to private hospitals or independent clinics operating under different EA permit frameworks — confirm your permit classification before selecting treatment technology.
Micro-example: An NHS trust commissioning an on-site SWH unit should begin the EA Environmental Permit application no later than 12 months before planned operational start. The pre-application consultation with the Environment Agency is strongly recommended before submitting a formal application. For the full EA permit application process, see our guide to UK on-site medical waste treatment permits and validation.
What Does a Side-by-Side Spec Sheet Look Like?
The table below compresses every decision-relevant parameter into a single comparison. SWH outperforms autoclaving on temperature, waste compatibility, residue value, and regulatory future-proofing.
| Parameter | Autoclave | PHANTOM SWH |
|---|---|---|
| Operating temperature | 121–134°C | ~200°C |
| Operating pressure | 1–3 bar | ~20 bar |
| Cycle time | 30–90 min | 30 min (0.5t/1t) · 45 min (2t/3t) |
| Available models | Various — multiple units for NHS scale | 0.5t · 1t · 2t · 3t per batch |
| Orange-stream infectious waste | ✓ Permitted | ✓ Treated |
| Prion-contaminated waste (CJD) | ✗ 134°C insufficient — prions resist steam | ✓ Higher temperature provides superior organic decomposition |
| Anatomical waste | ✗ Prohibited (HTM 07-01) | ✓ Hydrolysed within cycle |
| Pharmaceutical residues | ✗ APIs survive steam cycle | ✓ Hydrolysed (non-cytotoxic organic pharma) |
| Cytotoxic / cytostatic waste | ✗ Prohibited (HTM 07-01) | ⚠ Verify current EA guidance — confirm with your permit officer |
| Moisture sensitivity | High — wet loads risk log-kill shortfall at 60–75% moisture | None — pressurised liquid environment is moisture-neutral |
| Residue destination | Landfill (£126–£131/t tax) | Potential land application — zero landfill tax |
| Volume reduction | Minimal (shredding only) | Up to 80% mass reduction |
| Emissions | Steam venting; potential chemical aerosolisation | Zero — closed-loop, no combustion |
| UK ETS exposure (from 2028) | Excluded streams → incineration → ~+£48/t ETS uplift | No incineration required — no ETS exposure |
| EA permit required | No on-site permit for standard autoclave | EA Environmental Permit required (4–6 months) |
| Validation standard | BS EN 285 / EN 13060 | ISTAATT Level III — Log-6 reduction, HTM 07-01 equivalent |
| Revenue potential | None — residue is a cost | Sterile residue and liquid fraction have soil amendment value |

This applies when you need a single reference document for a procurement committee or board paper comparing these two technologies. It does not apply if you are comparing either technology to incineration alone — see the non-incineration medical waste treatment guide for that analysis.
Micro-example: A facilities director at a 600-bed teaching hospital presents this spec sheet to the trust's capital investment committee. The committee flags two rows — prion destruction and UK ETS exposure — as the deciding factors. The autoclave cannot address either. The PHANTOM organic waste treatment machine addresses both.
Pro-Tip: Why "Good Enough" Sterilisation Is the Most Expensive Decision in Clinical Waste
Choosing autoclaving because it is familiar costs more than choosing it because it is right. The root cause is not the technology — it is the assumption that sterilisation equals elimination. In my experience advising healthcare trusts on waste infrastructure procurement, the autoclave is always the first technology that reaches the shortlist. It is familiar, it is proven for standard infectious waste, and the capital cost is lower than most alternatives. That familiarity creates a blind spot.
Autoclaving sterilises waste. It does not eliminate it. Every tonne of autoclaved residue still exists physically, still occupies landfill capacity, and still carries a rising tax burden that will hit £130.75/t (~$166/t) from April 2026.
The 10% of waste streams that autoclaves cannot process — prions, cytotoxic compounds, pharmaceuticals — still ship to incineration at £500–£617/t. And from 2028, UK ETS carbon pricing will add another ~£48/t to every incineration invoice.
Subcritical water hydrolysis addresses the root cause. The PHANTOM organic waste treatment machine operates at 200°C and 20 bar — decomposing organic waste rather than merely sterilising it. The output is a sterile residue with soil amendment potential, not landfill-bound shredded waste. For a free feasibility assessment covering your facility's specific waste profile, throughput requirements, and 5-year TCO projection, speak to our team.
Frequently Asked Questions
No. Standard autoclaving at 134°C fails to completely denature prion proteins. CJD-contaminated material resists steam sterilisation and remains highly infectious post-treatment. Prion waste requires incineration or higher-temperature treatment.
200°C at 20 bar pressure — 66°C hotter than the maximum autoclave cycle. This triggers hydrolytic decomposition of organic compounds rather than surface sterilisation alone.
Landfill. Autoclaved waste is shredded and sterilised but retains its physical mass. UK landfill tax is £126.15/t (~$160/t) in 2025/26, rising to £130.75/t (~$166/t) from April 2026.
Indirectly, yes. The 10% of waste streams autoclaves cannot process still goes to incineration. From 2028, UK ETS will add approximately £48/t to incineration gate fees — a cost autoclave operators cannot avoid for their reject stream.
Both technologies complete a treatment cycle in approximately 30 minutes. SWH processes a broader range of waste streams per cycle, reducing the need for separate incineration contracts for pharmaceutical, cytotoxic, and prion-risk streams.
Sources: HTM 07-01 (NHS England, 2023 edition); GOV.UK Landfill Tax rates 2025–2027; HMRC OBR Autumn Budget 2024; UK Emissions Trading Scheme consultation documentation; industry incineration benchmarks (2025/26). Disposal rates based on UK industry averages.
Figures are for informational purposes only and do not constitute legal, financial, or procurement advice. ~1.27 USD/GBP.



