
Article Series

TL;DR — Hospital Single-Use Plastics & PPE Management
Hospitals can cut their single-use plastic waste by 20–40% without compromising patient safety by combining upstream source reduction with advanced downstream treatment.
A comprehensive hospital plastic reduction strategy requires three main interventions:
- Source Reduction: Eliminate clinically unnecessary PPE (e.g., implementing WHO "Gloves Off" protocols for routine care).
- Switch to Reusables: Transition from disposable blue wrap and gowns to EN 13795-1 certified reusable surgical textiles, which produce up to 84% less solid waste.
- Precision Segregation: Stop misclassifying non-infectious hygiene waste (like clean packaging and diapers) as regulated clinical waste.
- Zero-Emission Treatment: Use subcritical water hydrolysis at 150–250°C to sterilise and reduce the volume of residual infectious PPE without relying on incineration.
Applicable to: NHS trusts targeting the NHS Net Zero 2040 commitment, US hospitals under OSHA Bloodborne Pathogen Standard disposal obligations, and EU healthcare facilities under the EU Green Deal's circular economy targets — provided IPC protocols (HTM 07-01 in the UK) govern segregation decisions throughout.
Example: UCLA Medical Center saved $450,000/year by switching to reusable surgical gowns — a hospital that then routes its remaining infectious PPE through an on-site hydrolysis unit at ~$33 per cycle eliminates incineration's dioxin liability and off-site hauling costs in the same step.
Read the full guide below for lifecycle assessments of reusable textiles, WHO hand-hygiene data, and pathogen destruction capabilities of subcritical water. Related: Infectious Medical Waste: Non-Incineration Guide · UK On-Site Medical Waste: Permits & Validation
To see how single-use plastic management fits into the broader zero-emission disposal picture, explore our foundational resource: The Ultimate Guide to Zero-Emission Industrial Waste Treatment. For a complete guide to on-site system selection, throughput sizing, and ROI, see the PHANTOM organic waste treatment machine buyer's guide. Here, we focus on one of the most operationally complex waste challenges in any healthcare facility: single-use plastics and PPE — how to reduce them, how to manage what remains, and how to treat what cannot be eliminated.
Hospitals exist to heal. Yet the very infrastructure that protects patients — the gloves, gowns, syringes, incontinence products, IV bags, and sharps containers — generates a waste crisis of significant scale. The healthcare sector is responsible for 4.4–5.2% of global greenhouse gas emissions, and over 70% of that footprint is embedded in supply chains and discarded products. COVID-19 did not create this problem, but it compressed years of accumulated waste into months: an estimated 8.4 million tons of pandemic-associated plastic waste was generated globally by August 2021 alone, with 87.4% originating in hospitals (Peng et al., PNAS, 2021).
The core tension hospital administrators must resolve is not new, but it has become urgent: how do you maintain rigorous infection control while also meeting net-zero commitments, rising disposal costs, and tightening regulatory frameworks? The answer is not to choose between safety and sustainability — it is to apply engineering precision to both simultaneously.
US hospitals generate approximately 6 million tons of waste annually, with patients producing roughly 33.8 lbs (15.3 kg) of waste per day. Of this, 20–25% is plastic — roughly 1.7 million tonnes annually in the US alone (Rizan et al., Journal of the Royal Society of Medicine, February 2020). Commodity plastics (PE, PP, PVC, PS) comprise approximately 70% of medical devices by mass. For institutions already consulting the comprehensive guide to non-incineration medical waste treatment to understand disposal options, this article provides the upstream complement: reducing and reclassifying waste before it ever reaches a treatment system.
The Scale of the Problem
Sources: Peng et al., PNAS 2021 · Eunomia/Systemiq 2025 · Hsu et al., West J Emerg Med 2020 · AMA Journal of Ethics 2022phantomecotech.com
Why Do Hospitals Rely on Single-Use Plastics in the First Place?

Hospitals use single-use plastics primarily because they eliminate cross-contamination risk — but 85% of the plastic entering clinical waste bins does not meet the criteria for regulated medical waste and could legally be disposed of at far lower cost.
Four structural drivers of single-use plastic reliance in hospitals:
- Infection control requirements — sterility guaranteed for single-use; reprocessing at ward level cannot replicate this for all item types
- Regulatory liability — NHS litigation risk on reprocessing failures drives conservative procurement defaults
- Perceived cost advantage — unit cost of disposables appears lower than reprocessing overhead on a per-item basis
- Supply chain convenience — disposables are standardised, globally available, and JIT-compatible
Applies to: All acute NHS trusts and private hospitals. Does NOT apply to primary care or GP settings, where PPE volumes are substantially lower and reusable options dominate the infection control toolkit.
Example: The AMA Journal of Ethics (October 2022) notes directly: there is "no compelling evidence that using single-use disposables reduces healthcare-acquired infections" compared to properly reprocessed reusables — making the infection control justification for 85% of single-use plastics clinically unsupported.
Despite this, the structural inertia is real. Plastic is lightweight, chemically inert, sterilizable at low cost, and available through deeply optimised procurement channels. The clinical landscape includes disposal syringes (PP/PE), IV bags and blood tubing (PVC — approximately 40% of hospital waste in some audits), surgical wrap or "blue wrap" (polypropylene — approximately 255 million pounds discarded annually in the US), isolation gowns (PP non-woven — over 80% are disposable in US hospitals), gloves (nitrile, latex, vinyl — global consumption exceeds 50+ billion pairs annually), and disposable procedure packs containing combinations of all of the above.
A German hospital study found that PP alone constituted 45% of total plastic consumables by mass (Ivanovic et al., 2022). The operating theatre is the most plastic-intensive zone: it generates 30–35% of total hospital waste and produces two-thirds of regulated medical waste (Practice Greenhealth). It is also where the most dramatic reductions are achievable.
The AMA Journal of Ethics (October 2022) notes directly: there is "no compelling evidence that using single-use disposables reduces healthcare-acquired infections" compared to properly reprocessed reusables. The "single-use is safer" assumption is a myth embedded in procurement culture — not clinical science.
Strategy 1 — Source Reduction and the "Gloves Off" Principle
Between 33% and 59% of hospital glove use is clinically unnecessary. Eliminating non-indicated glove use is the fastest, lowest-cost waste reduction intervention available — and WHO now formally endorses it.
The data is unambiguous. Wilson, Bak & Loveday (2017) observed 278 procedures across two NHS hospitals and found gloves were inappropriate in 59% of cases, with cross-contamination risk present in 49% of care episodes (American Journal of Infection Control, 45(7):779–786). Earlier audits documented 42% overuse rates with a documented inverse relationship between glove use and hand hygiene compliance.
On World Hand Hygiene Day 2025 (May 5), WHO published its formal position: "Gloves do not replace hand hygiene." The WHO Glove Use Information Leaflet specifies that gloves should NOT be worn for routine patient care where no blood or body fluid contact is anticipated.
NHS "Gloves Off" campaigns demonstrate what precision targeting achieves without infection risk:
- Great Ormond Street Hospital: 18.3% reduction in weekly glove orders, saving 21 tonnes of plastic annually. No increase in hospital-acquired infections.
- Manchester Foundation Trust: 14.6% reduction, eliminating 11 million gloves (40 tonnes of plastic), saving 286 tonnes CO₂e and £14,000 (~$18,000 USD) annually.
- UCLH: Projected savings of at least £200,000 (~$254,000 USD) over 12 months.
- US outpatient (731-bed hospital): 27% reduction, saving 56,628 gloves and 180 kg of waste (Lalakea et al., OTO Open, 2025, PMC11950148).
In the US context, approximately 100–124 billion exam gloves are used annually, generating 350,000–434,000 tons of waste and 2.6–3.9 million metric tons of CO₂e. A 15% system-wide reduction would eliminate approximately 50,000 tonnes of waste — equivalent to removing hundreds of millions of dollars from disposal budgets.
Source reduction applies beyond gloves. Non-clinical zones — administrative areas, catering, outpatient reception — routinely use clinical-grade packaging and disposal pathways they do not require. A structured audit of all single-use plastic use by zone and function typically reveals 20–30% of usage that can be eliminated without any clinical impact.
Strategy 2 — Transitioning to Reusable Medical Textiles

Lifecycle assessments consistently show reusable surgical gowns and drapes produce 64–84% less environmental impact across energy, carbon, water, and solid waste metrics compared to disposables — at lower long-term cost — and meet identical infection control standards.
The "reusable is less sterile" myth persists in procurement culture despite conclusive evidence to the contrary. EN 13795-1:2019 (European Standard for surgical gowns, drapes, and clean air suits) defines performance levels for liquid-barrier protection, bacterial penetration resistance (wet and dry), burst and tensile strength, and linting — parameters that properly industrial-laundered reusables consistently meet or exceed. Kilinc-Balci et al. (2020) confirmed reusable gowns maintained full AAMI PB70 compliance through 75 industrial wash cycles while disposable gowns at all AAMI levels failed ASTM crosswise breaking strength requirements (American Journal of Infection Control, 2020, PMC7572274).
The environmental data from lifecycle assessments is decisive:
- Vozzola, Overcash & Griffing (2020, AORN Journal): Reusable surgical gowns (75-wash lifecycle) vs disposable — 64% less energy, 66% less GHG, 83% less water, 84% less solid waste.
- Overcash et al. (2012, Anesthesia & Analgesia): Six LCA studies — reusables use 2–3× less energy and water, produce 2–3× less carbon, and 7.5× less solid waste.
- Nieuwenhuizen et al. (BJOG, 2024): Manufacturing 1,000 disposable gowns produces ~1,495 kg CO₂e; 1,000 uses of reusable gowns produce ~143 kg CO₂e — a 10× carbon difference.
On cost, UCSF saved 2 cents per gown use while avoiding over 30,000 lbs of annual solid waste. Staff satisfaction rose from 22.9% to 58.3% (JAMA Network Open, 2023). UCLA Medical Center saves approximately $450,000 annually from reusable gown adoption.
The practical consideration is laundry logistics. Industrial healthcare laundry to EN 14065 (RABC — Risk Analysis Biocontamination Control) standards ensures full decontamination between uses. EN 14065 is auditable, documentable, and fully compatible with ISO 13485 quality management for medical devices. Hospitals without in-house laundry facilities can access validated third-party textile service providers across most markets.
Strategy 3 — Precision Waste Segregation and the True Cost of Misclassification
Up to 85% of waste in hospital clinical bins does not meet the criteria for regulated medical waste. This single misclassification error inflates disposal costs by up to 10× and is the most actionable near-term lever for budget reduction.
The NHS Clinical Waste Strategy (March 2023) introduced the 20:20:60 segregation target — only 20% of clinical waste to high-temperature incineration, 20% to alternative treatment (such as autoclaving), and 60% reclassified as offensive/hygiene waste — and calculated that achieving it would save £11 million (~$14 million USD) annually while cutting 29,540 tonnes CO₂e across the NHS. Barts Health NHS Trust demonstrated this is achievable in practice, increasing recycling from 11% to over 30% in 10 weeks and saving £1.2 million (~$1.5 million USD) annually (NHS SBS, 2024).
The UK colour-coded clinical waste system under HTM 07-01 (2022 edition) defines:
| Container | Colour | Classification | Treatment |
|---|---|---|---|
| Yellow bag/bin | Yellow | Infectious, requiring incineration (EWC 18 01 03*) | High-temperature incineration |
| Orange bag | Orange | Infectious, suitable for alternative treatment | Autoclave or equivalent |
| Tiger bag | Yellow/black stripe | Offensive/hygiene (non-infectious) — incontinence pads, non-infectious PPE | Energy-from-waste / deep landfill |
| Red bag/bin | Red | Anatomical waste | Incineration |
| Purple bin | Purple | Cytotoxic/cytostatic waste | Licensed incineration |
| Black bag | Black | General domestic waste | Municipal waste stream |
The critical insight: used incontinence products (diapers, continence pads), non-soiled PPE, and packaging from sterile items are offensive/hygiene waste — not infectious clinical waste. Their EWC code is 18 01 04 (non-hazardous), and they are legally and safely disposed of as tiger bag waste at a fraction of the cost of incineration. For nursing homes and care facilities where incontinence waste is the dominant stream, our dedicated guide to nursing home diaper disposal cost reduction covers the classification decision in detail and quantifies the full ROI case for on-site hydrolysis treatment.
Hsu et al. (2020, PMC7514403) conducted a physical audit of red biohazard bags in a US Level I trauma centre emergency department and found that 85% of bag contents did not meet the criteria for regulated medical waste. The CDC recommends regulated medical waste should constitute 3–5% of total hospital waste; in many US facilities it is approximately 15% — creating unnecessary disposal costs of approximately $400–800 per tonne above what is required.
Is Your Hospital Over-Classifying Clinical Waste?
Check each waste stream your facility currently routes to yellow bag (incineration). If any item below is going into a yellow bag, you are over-classifying — and over-paying.
Establishing an In-Hospital Circular Loop for Non-Infectious Plastics
Non-infectious plastics — IV bags (PVC), HDPE Tyvek packaging, PP procedure trays, polystyrene specimen containers, PET bottles — are technically recyclable and should never enter infectious waste streams. Practice Greenhealth estimates that 64% of operating theatre plastics are technically recyclable; in practice, less than 5% of healthcare plastics are recycled (Eunomia/Systemiq, 2025).
Building an in-hospital collection programme requires: (1) clear visual bin labelling and staff training on what constitutes non-infectious clinical plastic, (2) a clean collection point in each ward and department, (3) contracts with healthcare-specific plastic recyclers who can handle PVC (which requires specialist recycling due to chlorine content), and (4) a documented chain of custody to demonstrate regulatory compliance.
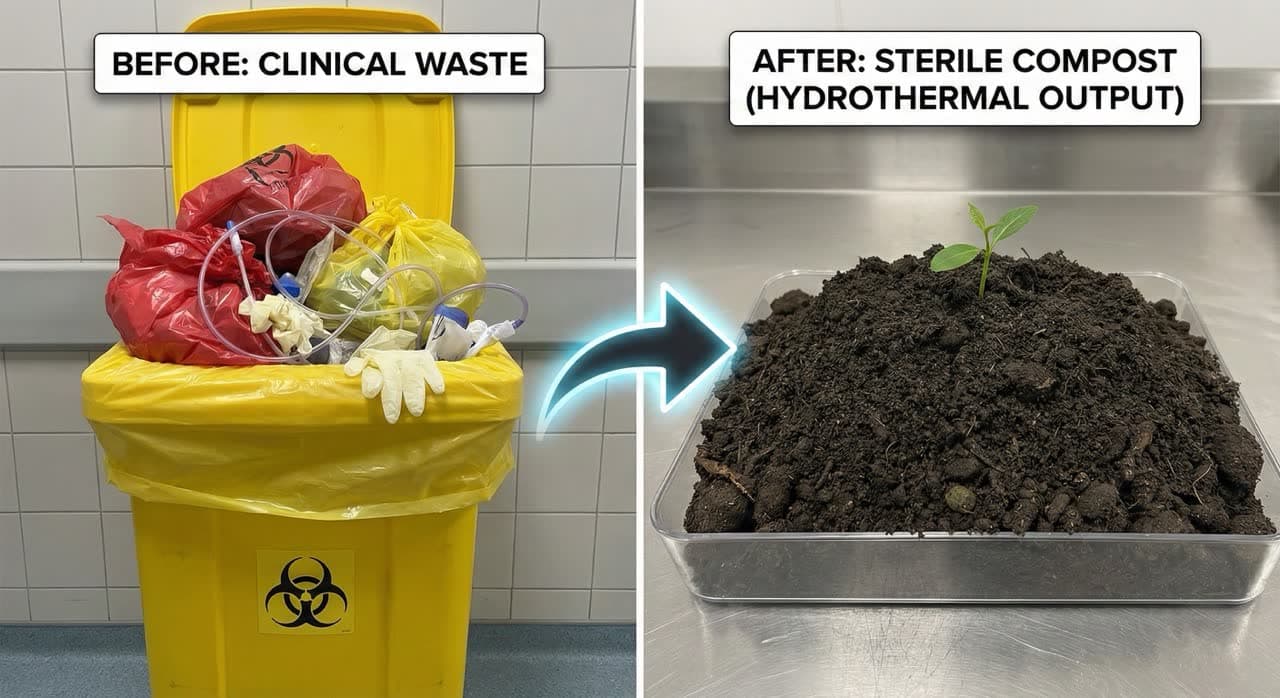
The Technology Layer — How Subcritical Water Hydrolysis Handles What Incineration Cannot
For infectious medical waste that cannot be recycled or reused — contaminated sharps containers, soiled incontinence products, blood-contaminated PPE, and mixed clinical waste — subcritical water hydrolysis achieves complete pathogen destruction, significant volume reduction (80–90% for dry PPE inputs), zero toxic emissions, and recoverable output materials.
For hospitals generating 500kg or more of residual infectious PPE and single-use plastics per week, the PHANTOM organic waste treatment machine is sized specifically for this throughput — eliminating incineration contracts and off-site hauling in a single operational step.
To understand why this technology is superior to incineration for mixed medical waste, the thermodynamics must be examined precisely.
Subcritical water (SCW) technology — often referred to as advanced hydrothermal treatment — operates at 100–374°C under sufficient pressure (typically 0.5–22 MPa) to maintain water in its liquid state, which radically alters its chemical properties. At these conditions, water's ionic product increases by three orders of magnitude, enabling it to act as both an acid and base catalyst — driving hydrolysis reactions without added chemicals (ACS Analytical Chemistry, 2016). The dielectric constant drops, allowing water to dissolve non-polar compounds similarly to organic solvents.

Pathogen Destruction: The Thermal Kill Data
For technical specifications relevant to hospital administrators evaluating treatment options, optimal pathogen destruction typically requires a practical operating window of 150–250°C at 0.5–4 MPa with 30–120 minute residence times (MDPI Energies, 14(23):8065, 2021). At these temperatures — far exceeding what is needed to destroy even the most resistant hospital pathogens including C. difficile spores (121°C) and HBV (98°C) — all known pathogens are reliably destroyed.
Compare PHANTOM's operating range against the thermal destruction requirements for key hospital pathogens:
| Pathogen | Minimum Destruction Requirement | PHANTOM Operating Range |
|---|---|---|
| MRSA (vegetative) | 70°C / 30 min OR 121°C / instant | 150–250°C ✓ |
| C. difficile spores | 121°C / 15–30 min (moist heat) | 150–250°C ✓ |
| Hepatitis B (HBV) | >98°C / 5 min | 150–250°C ✓ |
| Hepatitis C (HCV) | 65°C / 4 min | 150–250°C ✓ |
| HIV | 56°C / 30 min | 150–250°C ✓ |
| Prions (CJD) | 134°C / 18 min (steam) | 150–250°C ✓ |
All pathogen classes — bacteria, spores, viruses, fungi, parasites — are destroyed at PHANTOM operating temperatures. The log-6 kill standard (99.9999% microbial reduction) required for medical waste is achieved with significant margin.
Treatment Technology vs. Pathogen Destruction
Required temperatures for hospital pathogen classes vs. PHANTOM's operating range
| Pathogen | Min. Kill Temp. | Autoclave (121°C) | PHANTOM (150–250°C) | Incineration (>850°C) |
|---|---|---|---|---|
| MRSA | 70°C / 30 min | ✓ | ✓ | ✓ |
| C. difficile spores | 121°C / 15–30 min | ⚠ Marginal | ✓ | ✓ |
| Hepatitis B (HBV) | ≥98°C / 5 min | ✓ | ✓ | ✓ |
| HIV | 56°C / 30 min | ✓ | ✓ | ✓ |
| Prions (CJD) | 134°C / 18 min (steam) | ✗ Standard fails | ✓ | ✓ |
| PVC Dioxin production | N/A — emission concern | ✓ None | ✓ None 83–95% dechlorination | ✗ Produces dioxins |
What Happens to Hospital Waste Streams Inside a PHANTOM Unit
Contaminated diapers and incontinence products: The cellulose, polymer superabsorbent, and cotton fibre matrix hydrolyses into low-molecular-weight organic compounds. The resulting output is sterile, deodorised compost-grade material suitable for agricultural application. Volume is reduced by approximately 60% through the hydrolysis process.
Bloodborne pathogen-contaminated PPE (gowns, gloves, masks, face shields): Polymer chains in PP, PE, and nitrile are fragmented under subcritical water conditions. Pathogen load is eliminated. The residual material — depending on input composition — can be directed toward fuel pellet production or composting. HTC of surgical masks achieves up to 75% volume reduction with hydrochar HHV of 24.2 MJ/kg (MDPI Sustainability, 15(12):9382, 2023).
Used sharps containers: The PP container material undergoes hydrolysis. The metallic sharps (needles, lancets) pass through as inorganic residue — unchanged, but fully sterile and safely separated for metal recycling. Glass, metal, and stone cannot be processed by PHANTOM and exit as inorganic residue.
Soiled incontinence products (used diapers): Cellulosic and polymer components hydrolyse. Output is deodorised and sterile organic matter. The PHANTOM 3M3 specification handles input loads of up to 3 tonnes per cycle, yielding approximately 1.8 tonnes of output — a 40% mass reduction relative to wet input weight. Facility directors should note that for high-moisture inputs like wet diapers, mass reduction is governed by moisture content rather than polymer breakdown. The operational value here is sterilisation, deodorisation, and safe volume compaction of a biohazardous waste stream into manageable, compost-suitable output. For dry inputs such as gowns, gloves, and masks, volume reduction of 80–90% is achievable (MDPI Sustainability, 15(12):9382, 2023; PMC9419444).
A critical environmental advantage over incineration: subcritical water processes produce no dioxins, furans, NOx, mercury, or persistent organic pollutants. Incineration of PPE waste produces approximately 1,074 kg CO₂e per tonne (PMC9419444). For PVC-containing medical waste specifically, HTC at 220–300°C achieves 83–95% dechlorination efficiency, eliminating the dioxin precursor problem that makes PVC incineration hazardous (Journal of Hazardous Materials, 2019).
Green Procurement — Changing the Waste Problem Upstream
Over 70% of healthcare's greenhouse gas emissions originate in the supply chain. Green procurement is not a CSR initiative — it is the dominant engineering lever for decarbonisation.

Procurement data from the NHS is instructive: 62% of the NHS's total carbon footprint is attributable to approximately 80,000 suppliers. The NHS became the world's first health system to commit to net zero in October 2020, and its Net Zero Supplier Roadmap now mandates escalating requirements: a minimum 10% net zero weighting in all procurements from April 2022; mandatory Carbon Reduction Plans for contracts above £5 million (~$6.4 million USD) from April 2023; mandatory product-level carbon footprinting from April 2028.
For hospital administrators, this translates into practical supplier evaluation criteria: total lifecycle carbon per unit (not just purchase price), end-of-life recyclability, packaging reduction commitments, reusable textile programme availability, and ISO 14001 certification of manufacturing sites.
Key frameworks and resources include Health Care Without Harm's Sustainable Procurement Guide, Practice Greenhealth's Greenhealth Approved Seal and Exchange marketplace (serving 1,500+ US hospitals), and ISO 14001:2015 environmental management certification for supply chain partners. Real-world savings are substantial: UCLA Medical Center saved approximately $450,000/year by transitioning to reusable isolation gowns; Cleveland Clinic saved more than $100 million since 2010 through energy efficiency; Gundersen Health System accumulates $3 million in annual sustainability savings (GHX Healthcare Hub; HCWH).
What a 3-Year Waste Optimisation Programme Delivers
Illustrative for a 500-bed hospital. Actual results vary by facility.
Overcoming Barriers — Training, Culture, and Behaviour Change
The largest gap between policy and practice in hospital waste management is not technical — it is behavioural. Staff knowledge, visual cueing, and transparent waste data are the three most effective levers for closing it.
Research consistently shows that healthcare workers misclassify waste not out of negligence, but because bin placement, labelling ambiguity, and time pressure make correct segregation difficult at point-of-care. A 2025 simulation study published in Perioperative Medicine (Biomedcentral) found that nudge interventions — repositioning waste bins, adding decision prompts, and using visual colour cues at point of use — reduced misclassification rates by approximately 30% without additional training.
Effective change programmes share three characteristics:
Data transparency: Show department-level waste volumes and costs weekly. Waste cost dashboards surfaced to ward managers and department heads create accountability. Facilities that make waste data visible — cost per patient admission, cost per procedure, proportion incorrectly classified — consistently report faster behavioural change.
Visual decision support: Every bin point should provide a decision tree, not just a colour. "Does this item have visible blood or body fluid? → Yes: Orange bag. No: Tiger bag." Decision logic at point-of-care reduces cognitive burden and eliminates the default to "when in doubt, throw yellow."
Structured training with clinical validity: Training that frames waste reduction as an infection control improvement — not a compromise — achieves significantly higher compliance. The NHS "Gloves Off" campaigns succeeded in part because they were led by Infection Prevention and Control teams, not facilities managers. When the message is that proper glove use is better infection control, clinicians engage.
Conclusion — Towards Net-Zero Healthcare Without Compromising Patient Safety
The evidence on which this article is built points to a clear conclusion: hospital waste management is simultaneously a patient safety issue, a regulatory compliance issue, and a financial management issue — and the interventions that improve one dimension typically improve all three. For a rigorous 10-year total cost of ownership comparison of autoclave vs. incineration vs. hydrolysis across UK, EU, and GCC markets, see our dedicated TCO breakdown.
The core strategy is engineering precision applied at each stage of the waste lifecycle. Reduction at source (glove optimisation, non-clinical plastic elimination) eliminates 15–27% of volume before it enters the waste stream. Transition to reusable surgical textiles eliminates up to 84% of solid waste from the most intensive clinical zones. Precision segregation reclassifies 40–60% of waste from expensive incineration streams to lower-cost treatment. And for the residual infectious waste that cannot be reduced, reused, or reclassified — subcritical water hydrolysis offers a technically superior, zero-emission alternative to incineration.
The evidence points to several actionable conclusions for hospital administrators. First, the waste problem is substantially self-inflicted: up to 85% of waste in clinical bins is misclassified, and proper segregation alone could cut waste costs by 20–40% and carbon emissions by 30%. Second, glove use reduction of 15–27% is safely achievable without infection risk, backed by WHO endorsement and multiple NHS demonstrations. Third, reusable surgical gowns and drapes are cheaper, stronger, and produce 2–7.5× less environmental impact across every metric compared to disposables. Fourth, subcritical water hydrolysis offers a technically superior alternative to incineration — achieving pathogen destruction at temperatures well above what is needed for even the most resistant hospital organisms, eliminating toxic emissions, and delivering 80–90% volume reduction for dry PPE waste streams. Finally, procurement is the dominant lever: with 62–70% of healthcare emissions embedded in the supply chain, green procurement frameworks represent the highest-impact intervention available to any hospital system serious about sustainability.
Environmental sustainability and infection control are not a zero-sum tradeoff. The data says they are complementary. The question for hospital administrators is not whether to act, but where to begin.
For institutions ready to implement these changes, calculate your facility's ROI on the PHANTOM machine page or contact Phantom for a site-specific waste audit and technology assessment.
Frequently Asked Questions
Infection control remains the fundamental constraint. Truly single-use items — needles, IV catheters, sterile procedure kits — prevent pathogen transmission between patients in ways that cannot be replicated by reprocessing at ward level. The target is not total elimination but structured reduction: eliminating non-indicated use, substituting reusables where clinical equivalence is established, and treating the genuinely single-use residual with the most appropriate technology.
Yes, when laundered to EN 14065 (RABC) standards by validated industrial laundry providers. EN 13795-1:2019 sets identical performance criteria for both reusable and disposable gowns — liquid barrier resistance, bacterial penetration, burst strength — and reusables consistently meet High Performance level through 75+ wash cycles (Kilinc-Balci et al., 2020, American Journal of Infection Control, PMC7572274).
PPE visibly contaminated with blood, body fluids, or contact with infectious patients falls under EWC 18 01 03* (UK/EU) or OSHA regulated waste (US) and cannot enter standard plastic recycling streams. It requires treatment — by incineration, alternative treatment (autoclaving, hydrothermal processing), or chemical disinfection — before any material recovery. Subcritical water hydrolysis is one of the few technologies that achieves both pathogen destruction and material recovery (as fuel or compost) in a single step.
In the short term, capital investment in reusable textile programmes (laundry equipment or contracts) requires upfront commitment. Across a 2–3 year horizon, the combination of reduced procurement volume (reusables vs. continuous disposable purchasing), lower disposal costs (tiger bag vs. incineration per tonne), and carbon compliance avoidance consistently produces net savings. UCLA Medical Center's $450,000 annual saving from reusable gown adoption is a representative outcome at scale.
In healthcare context, circular economy thinking replaces the linear "manufacture → use → incinerate" model with closed loops: reusable textiles returned to service after validated cleaning; non-infectious packaging plastics collected and recycled; organic clinical waste (incontinence products, food waste) hydrolysed into compost or biogas feedstock; residual infectious waste converted into sterile fuel material rather than emitting CO₂ and toxins through incineration. Subcritical water hydrolysis enables the final stage of this loop — converting unavoidable clinical waste into recoverable resources.
Key Sources & Citations: Peng et al., PNAS 2021 · Rizan et al., Journal of the Royal Society of Medicine 2020 · Wilson, Bak & Loveday, AJIC 2017 · WHO Glove Use Information Leaflet 2025 · Lalakea et al., OTO Open 2025 · Vozzola, Overcash & Griffing, AORN Journal 2020 · Kilinc-Balci et al., AJIC 2020 · Nieuwenhuizen et al., BJOG 2024 · NHS Clinical Waste Strategy March 2023 · NHS SBS Barts Health 2024 · Hsu et al., West J Emerg Med 2020 · ACS Analytical Chemistry 2016 · MDPI Energies 14(23):8065 2021 · MDPI Sustainability 15(12):9382 2023 · Journal of Hazardous Materials 2019 · AMA Journal of Ethics October 2022 · Practice Greenhealth · Health Care Without Harm · Eunomia/Systemiq 2025
⚠️ Disclaimer: The information in this article is for general informational purposes only and does not constitute legal, regulatory, or financial advice. Cost projections, compliance guidance, and technology comparisons are illustrative and based on publicly available data and operator-reported figures. Actual results will vary based on facility type, waste volumes, and regional regulations. Always seek qualified professional advice and verify compliance with applicable local, national, and international standards before implementing any waste management programme.


